Authorization Representative Form
Authorization Representative Form - Use this form to appoint a representative to help you with your social security case. _________________________________________________________ to act as my authorized representative. Download the form and follow these steps to fill out an appoint an authorized representative for my appeal form online. This individual is an adult who is sufficiently aware. You can submit this form if you would like to designate an authorized representative to act on your behalf. If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. By choosing an authorized representative, you or your legal representative agree your authorized representative can act on your behalf for the.
This individual is an adult who is sufficiently aware. Use this form to appoint a representative to help you with your social security case. By choosing an authorized representative, you or your legal representative agree your authorized representative can act on your behalf for the. Download the form and follow these steps to fill out an appoint an authorized representative for my appeal form online. You can submit this form if you would like to designate an authorized representative to act on your behalf. If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. _________________________________________________________ to act as my authorized representative.
You can submit this form if you would like to designate an authorized representative to act on your behalf. By choosing an authorized representative, you or your legal representative agree your authorized representative can act on your behalf for the. _________________________________________________________ to act as my authorized representative. Use this form to appoint a representative to help you with your social security case. If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. This individual is an adult who is sufficiently aware. Download the form and follow these steps to fill out an appoint an authorized representative for my appeal form online.
46 Authorization Letter Samples & Templates ᐅ TemplateLab
This individual is an adult who is sufficiently aware. _________________________________________________________ to act as my authorized representative. Use this form to appoint a representative to help you with your social security case. By choosing an authorized representative, you or your legal representative agree your authorized representative can act on your behalf for the. If you want someone to represent you concerning.
Authorization For Philhealth Signatories Representatives Form Fill
You can submit this form if you would like to designate an authorized representative to act on your behalf. If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. This individual is an adult who is sufficiently aware. _________________________________________________________ to act as my authorized representative. Use this form to appoint.
Uhc Designation Of Authorized Representative Form
If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. Download the form and follow these steps to fill out an appoint an authorized representative for my appeal form online. _________________________________________________________ to act as my authorized representative. By choosing an authorized representative, you or your legal representative agree your authorized.

Authorized Representative Form Sample Fill and Sign Printable
Download the form and follow these steps to fill out an appoint an authorized representative for my appeal form online. This individual is an adult who is sufficiently aware. _________________________________________________________ to act as my authorized representative. By choosing an authorized representative, you or your legal representative agree your authorized representative can act on your behalf for the. If you want.
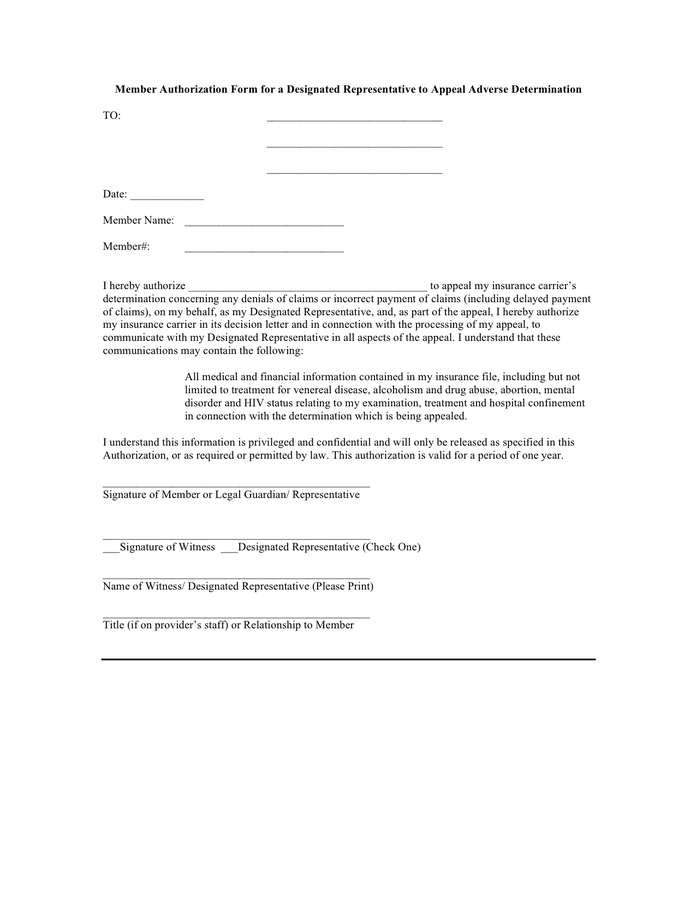
Member authorization form for a designated representative in Word and
Download the form and follow these steps to fill out an appoint an authorized representative for my appeal form online. You can submit this form if you would like to designate an authorized representative to act on your behalf. _________________________________________________________ to act as my authorized representative. By choosing an authorized representative, you or your legal representative agree your authorized representative.
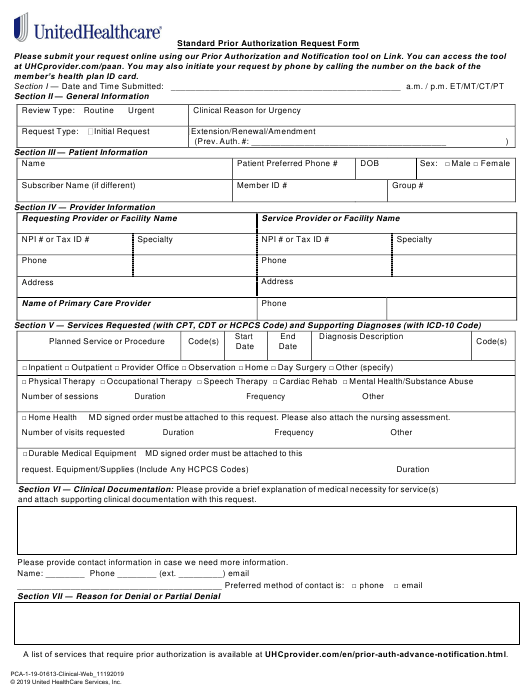
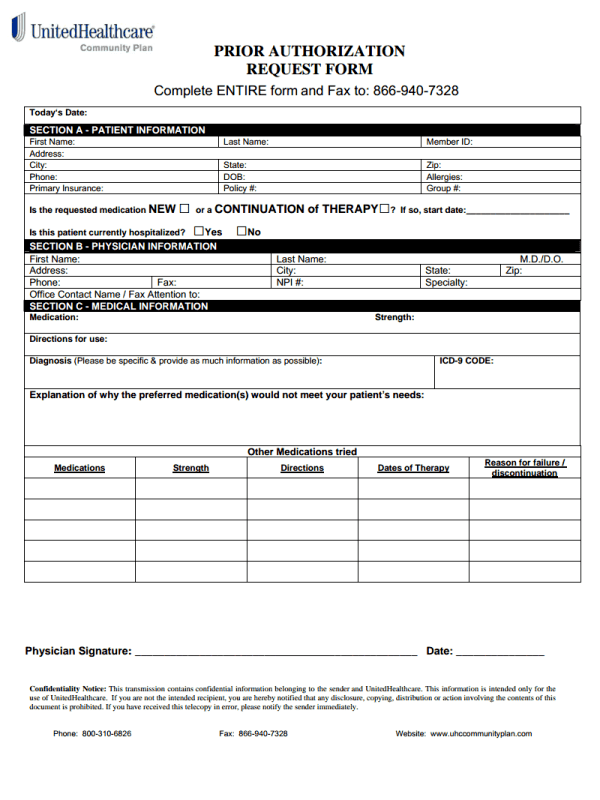
Unitedhealthcare Community Plan Prior Authorization Form Washington
_________________________________________________________ to act as my authorized representative. By choosing an authorized representative, you or your legal representative agree your authorized representative can act on your behalf for the. Use this form to appoint a representative to help you with your social security case. You can submit this form if you would like to designate an authorized representative to act on.
4+ Sample of Letter of Authorization to Represent in PDF Word(Docs)
You can submit this form if you would like to designate an authorized representative to act on your behalf. By choosing an authorized representative, you or your legal representative agree your authorized representative can act on your behalf for the. If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,..
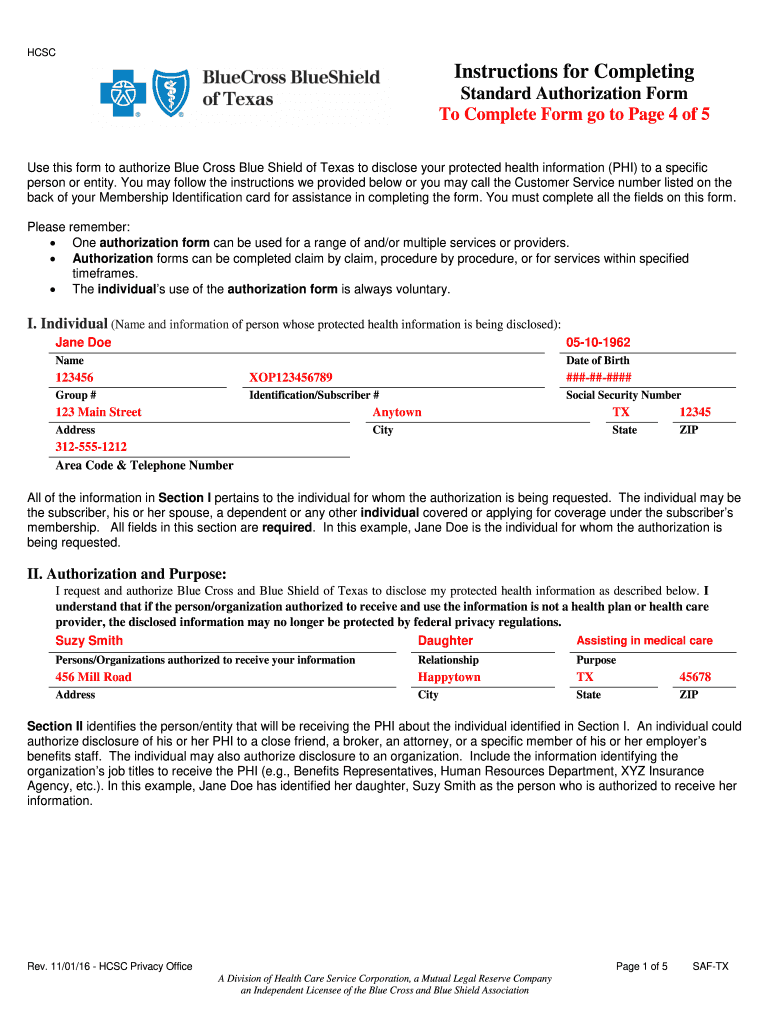
Bcbs standard authorization form Fill out & sign online DocHub
Use this form to appoint a representative to help you with your social security case. _________________________________________________________ to act as my authorized representative. You can submit this form if you would like to designate an authorized representative to act on your behalf. This individual is an adult who is sufficiently aware. If you want someone to represent you concerning services received.

Free Power of Attorney Authorization Letter Sample
You can submit this form if you would like to designate an authorized representative to act on your behalf. If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. Use this form to appoint a representative to help you with your social security case. Download the form and follow these.

PhilHealth Authorization Letter Format and Sample MattsCradle
By choosing an authorized representative, you or your legal representative agree your authorized representative can act on your behalf for the. This individual is an adult who is sufficiently aware. You can submit this form if you would like to designate an authorized representative to act on your behalf. Download the form and follow these steps to fill out an.
Download The Form And Follow These Steps To Fill Out An Appoint An Authorized Representative For My Appeal Form Online.
_________________________________________________________ to act as my authorized representative. By choosing an authorized representative, you or your legal representative agree your authorized representative can act on your behalf for the. This individual is an adult who is sufficiently aware. You can submit this form if you would like to designate an authorized representative to act on your behalf.
Use This Form To Appoint A Representative To Help You With Your Social Security Case.
If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,.