Hipaa Release Form Nc
Hipaa Release Form Nc - This information has been disclosed to you from records protected by federal confidentiality rules (42 cfr part 2). Prior to disclosing and exchanging specific health information from the records to and from particular individual(s) or agency(s), this. Consent for release of confidential. I authorize the named health care provider to release the information or records specified to north carolina league of municipalities upon. The board of law examiners of the state of north carolina is aware of hipaa requirements. Please send your completed authorization to use or disclose protected health information (phi) form by fax or mail to the entity listed below (if.
I authorize the named health care provider to release the information or records specified to north carolina league of municipalities upon. Please send your completed authorization to use or disclose protected health information (phi) form by fax or mail to the entity listed below (if. Consent for release of confidential. The board of law examiners of the state of north carolina is aware of hipaa requirements. Prior to disclosing and exchanging specific health information from the records to and from particular individual(s) or agency(s), this. This information has been disclosed to you from records protected by federal confidentiality rules (42 cfr part 2).
This information has been disclosed to you from records protected by federal confidentiality rules (42 cfr part 2). Prior to disclosing and exchanging specific health information from the records to and from particular individual(s) or agency(s), this. The board of law examiners of the state of north carolina is aware of hipaa requirements. I authorize the named health care provider to release the information or records specified to north carolina league of municipalities upon. Consent for release of confidential. Please send your completed authorization to use or disclose protected health information (phi) form by fax or mail to the entity listed below (if.

HIPAA Release Template
This information has been disclosed to you from records protected by federal confidentiality rules (42 cfr part 2). Consent for release of confidential. Please send your completed authorization to use or disclose protected health information (phi) form by fax or mail to the entity listed below (if. The board of law examiners of the state of north carolina is aware.

Hipaa Release Of Information Form To Family
I authorize the named health care provider to release the information or records specified to north carolina league of municipalities upon. The board of law examiners of the state of north carolina is aware of hipaa requirements. Consent for release of confidential. This information has been disclosed to you from records protected by federal confidentiality rules (42 cfr part 2)..
Hipaa Form Authorization Washington State
This information has been disclosed to you from records protected by federal confidentiality rules (42 cfr part 2). Consent for release of confidential. The board of law examiners of the state of north carolina is aware of hipaa requirements. Prior to disclosing and exchanging specific health information from the records to and from particular individual(s) or agency(s), this. I authorize.
Hipaa Printable Forms
This information has been disclosed to you from records protected by federal confidentiality rules (42 cfr part 2). Consent for release of confidential. I authorize the named health care provider to release the information or records specified to north carolina league of municipalities upon. The board of law examiners of the state of north carolina is aware of hipaa requirements..

What is a HIPAA Release Form? Checklist & Templates
Please send your completed authorization to use or disclose protected health information (phi) form by fax or mail to the entity listed below (if. The board of law examiners of the state of north carolina is aware of hipaa requirements. Consent for release of confidential. I authorize the named health care provider to release the information or records specified to.
Printable Hipaa Release Form
I authorize the named health care provider to release the information or records specified to north carolina league of municipalities upon. Prior to disclosing and exchanging specific health information from the records to and from particular individual(s) or agency(s), this. Please send your completed authorization to use or disclose protected health information (phi) form by fax or mail to the.
Hippa Free Printable Form For Ohio Form Printable Forms Free Online
This information has been disclosed to you from records protected by federal confidentiality rules (42 cfr part 2). Please send your completed authorization to use or disclose protected health information (phi) form by fax or mail to the entity listed below (if. Prior to disclosing and exchanging specific health information from the records to and from particular individual(s) or agency(s),.
Hipaa Compliant Medical Release Form amulette
I authorize the named health care provider to release the information or records specified to north carolina league of municipalities upon. The board of law examiners of the state of north carolina is aware of hipaa requirements. Prior to disclosing and exchanging specific health information from the records to and from particular individual(s) or agency(s), this. This information has been.
Hipaa Printable Forms
The board of law examiners of the state of north carolina is aware of hipaa requirements. This information has been disclosed to you from records protected by federal confidentiality rules (42 cfr part 2). Consent for release of confidential. I authorize the named health care provider to release the information or records specified to north carolina league of municipalities upon..
Hipaa Free Printable Form For Ohio Form Printable Forms Free Online
This information has been disclosed to you from records protected by federal confidentiality rules (42 cfr part 2). Please send your completed authorization to use or disclose protected health information (phi) form by fax or mail to the entity listed below (if. The board of law examiners of the state of north carolina is aware of hipaa requirements. Consent for.
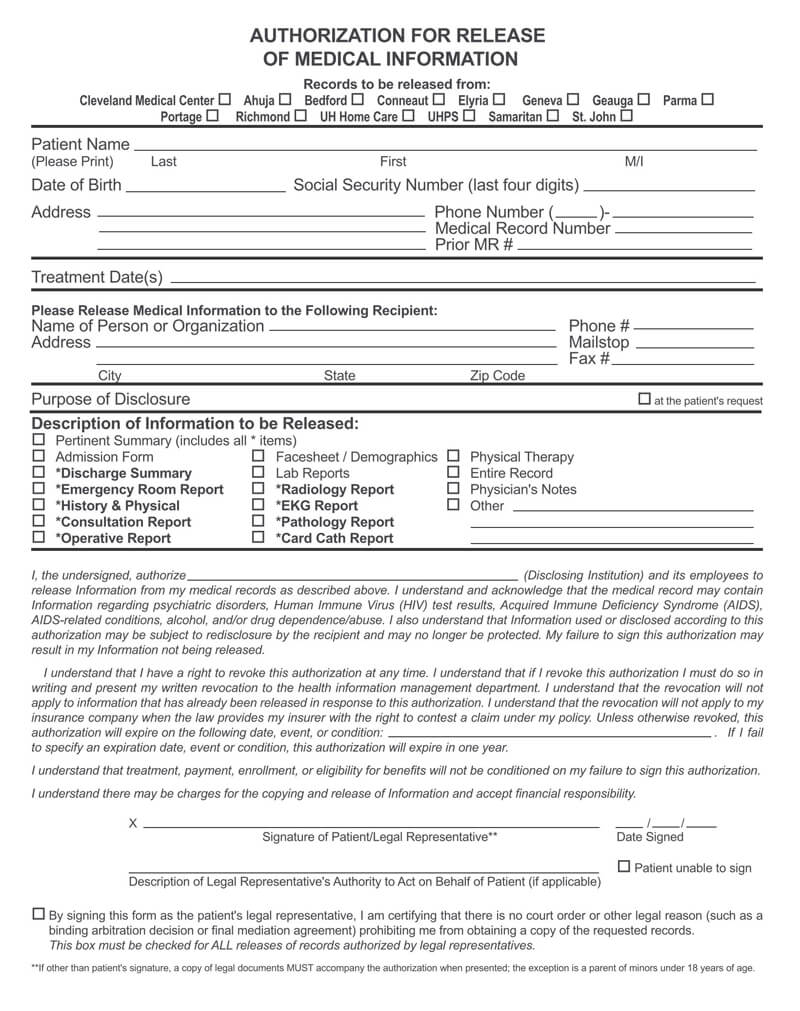
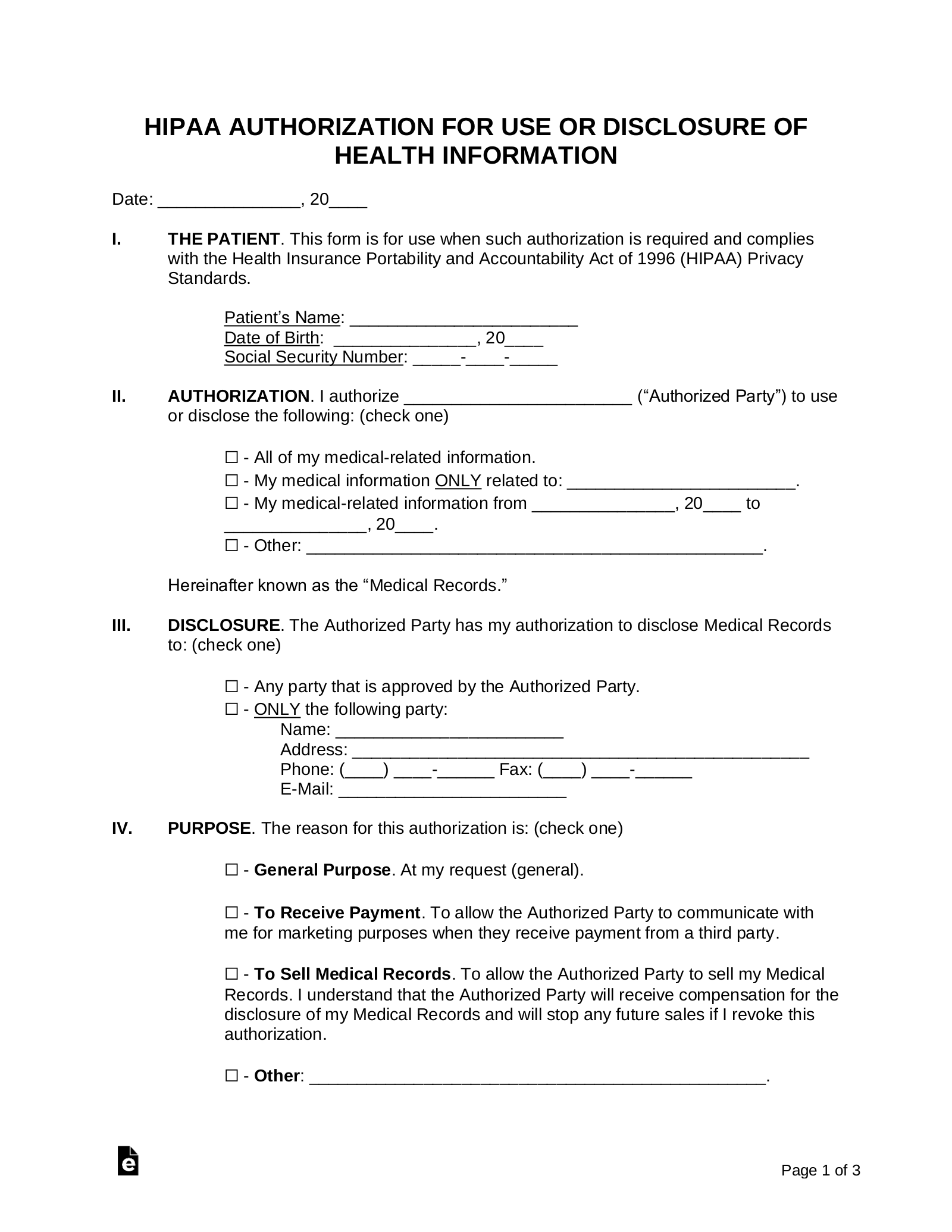
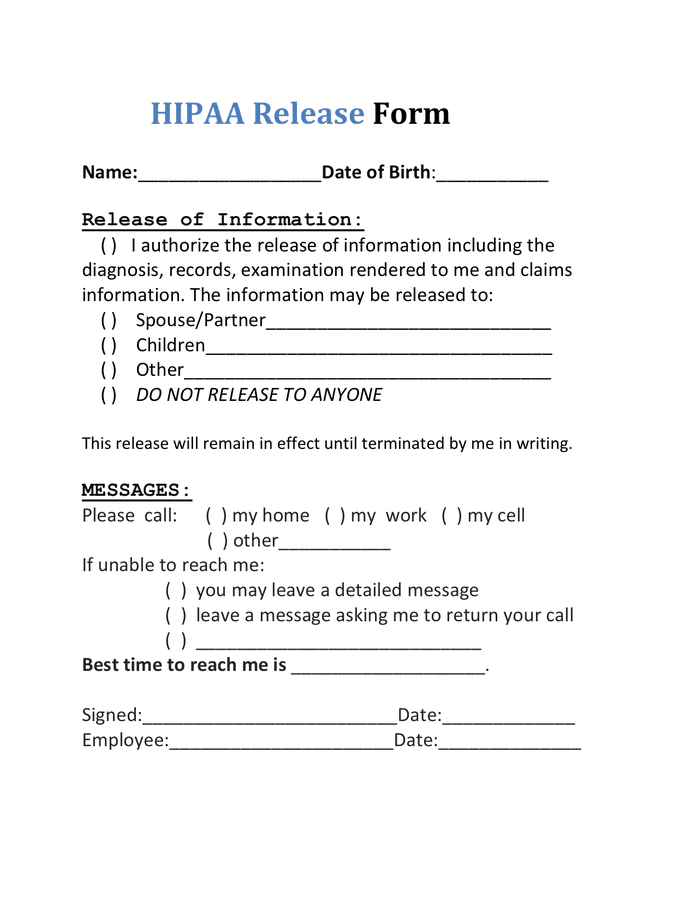
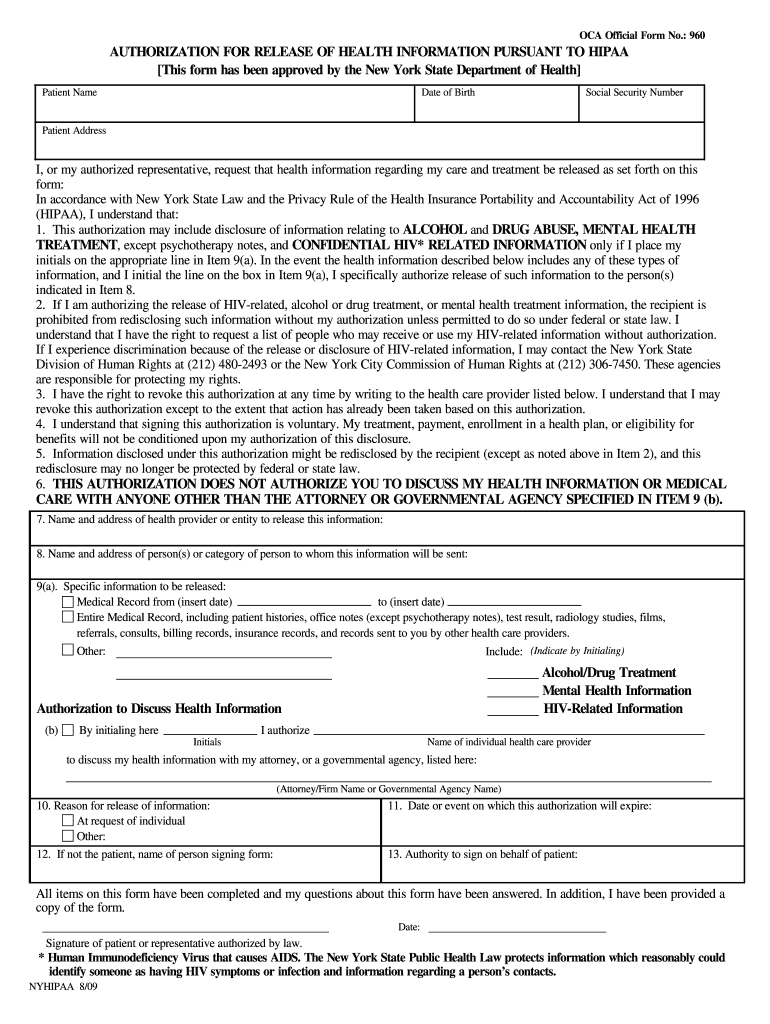
This Information Has Been Disclosed To You From Records Protected By Federal Confidentiality Rules (42 Cfr Part 2).
Consent for release of confidential. Please send your completed authorization to use or disclose protected health information (phi) form by fax or mail to the entity listed below (if. Prior to disclosing and exchanging specific health information from the records to and from particular individual(s) or agency(s), this. The board of law examiners of the state of north carolina is aware of hipaa requirements.