Pacific Health Alliance Prior Authorization Form
Pacific Health Alliance Prior Authorization Form - Your provider can request prior authorization from our health services department by fax, mail, or email. Find forms and resources to better work with us as you care for your patients. Po box 460351 san francisco, ca 94146 Use this form when requesting coverage for all drugs covered under either the pharmacy or medical benefit. Please complete the form in its. If the provider won’t request prior. To contact pha or avante behavioral health, please call:
Your provider can request prior authorization from our health services department by fax, mail, or email. To contact pha or avante behavioral health, please call: Use this form when requesting coverage for all drugs covered under either the pharmacy or medical benefit. Po box 460351 san francisco, ca 94146 Find forms and resources to better work with us as you care for your patients. Please complete the form in its. If the provider won’t request prior.
Find forms and resources to better work with us as you care for your patients. To contact pha or avante behavioral health, please call: Use this form when requesting coverage for all drugs covered under either the pharmacy or medical benefit. Please complete the form in its. If the provider won’t request prior. Po box 460351 san francisco, ca 94146 Your provider can request prior authorization from our health services department by fax, mail, or email.
Health First Health Plans Pharmacy Authorization Exception Form
Please complete the form in its. Find forms and resources to better work with us as you care for your patients. If the provider won’t request prior. Use this form when requesting coverage for all drugs covered under either the pharmacy or medical benefit. Po box 460351 san francisco, ca 94146

Medicaid Pre Authorization Form
Please complete the form in its. Po box 460351 san francisco, ca 94146 Find forms and resources to better work with us as you care for your patients. To contact pha or avante behavioral health, please call: If the provider won’t request prior.
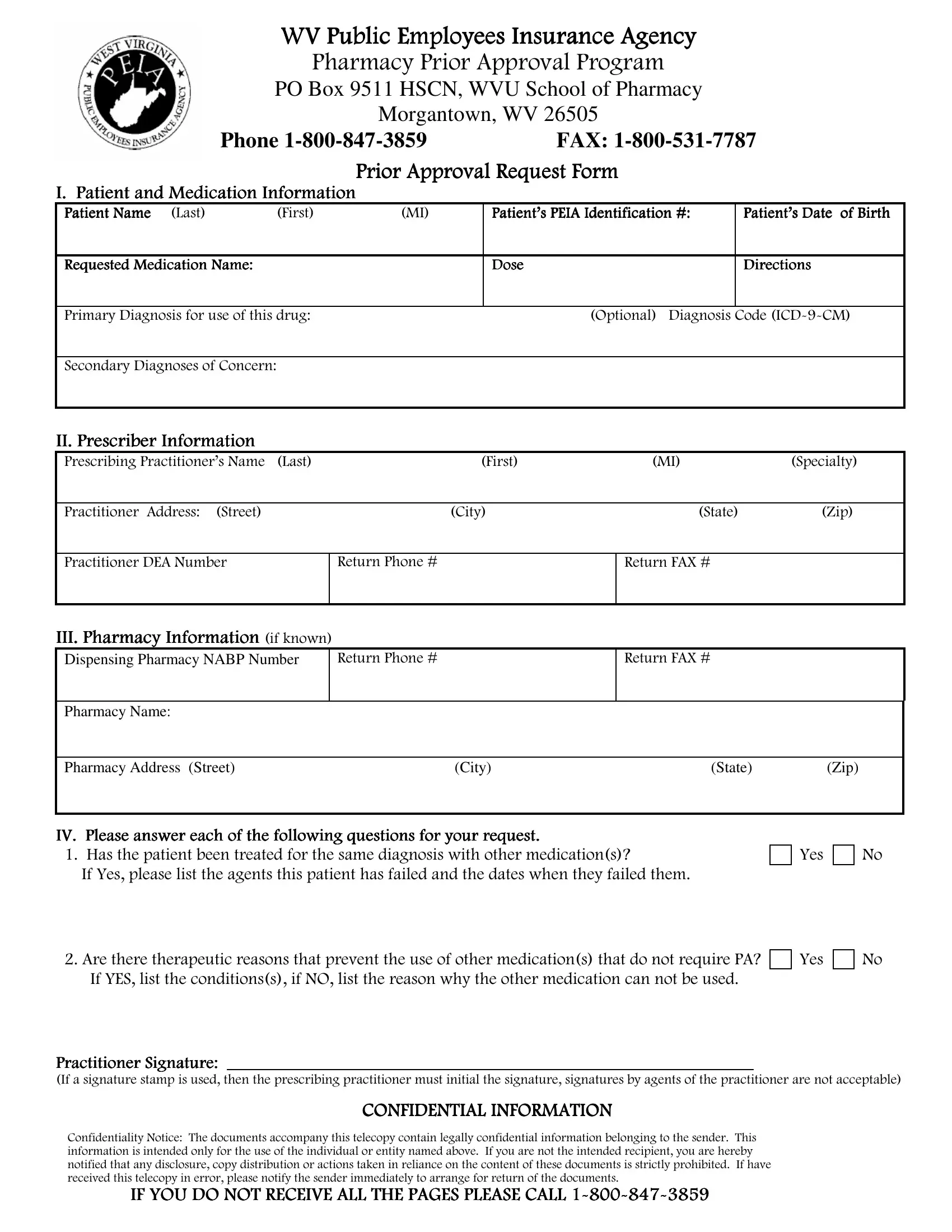
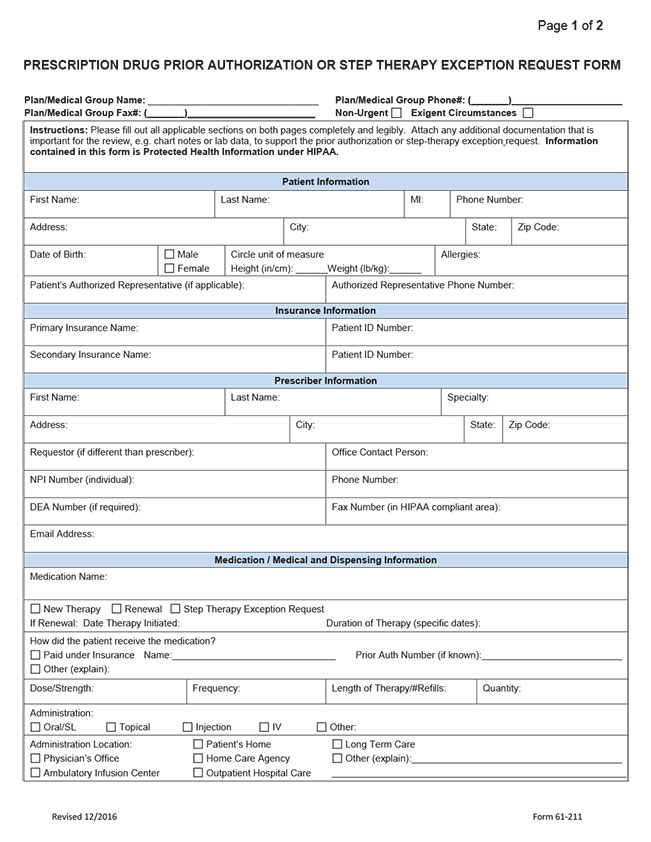
Wv Peia Prior Authorization PDF Form FormsPal
Po box 460351 san francisco, ca 94146 Your provider can request prior authorization from our health services department by fax, mail, or email. Find forms and resources to better work with us as you care for your patients. If the provider won’t request prior. Please complete the form in its.

Superior Health Plan Therapy Authorization Form
If the provider won’t request prior. Po box 460351 san francisco, ca 94146 Your provider can request prior authorization from our health services department by fax, mail, or email. Use this form when requesting coverage for all drugs covered under either the pharmacy or medical benefit. To contact pha or avante behavioral health, please call:
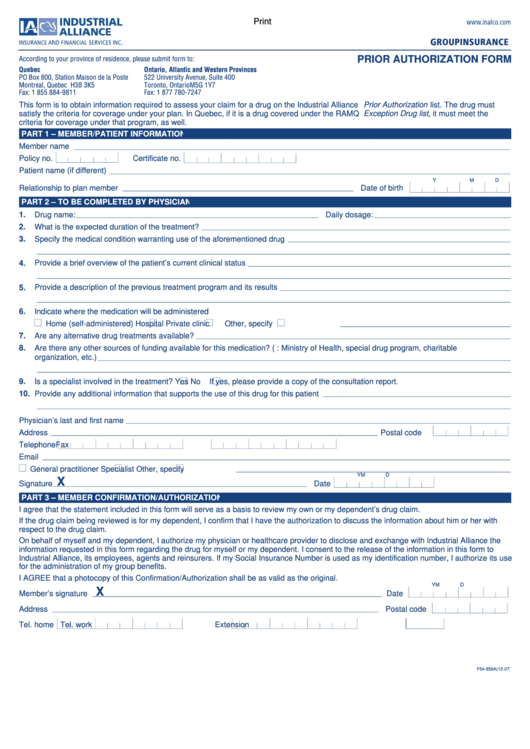
Fillable Industrial Alliance Prior Authorization Form printable pdf
Find forms and resources to better work with us as you care for your patients. If the provider won’t request prior. To contact pha or avante behavioral health, please call: Your provider can request prior authorization from our health services department by fax, mail, or email. Please complete the form in its.

Pacific health alliance auth form Fill out & sign online DocHub
To contact pha or avante behavioral health, please call: Please complete the form in its. Your provider can request prior authorization from our health services department by fax, mail, or email. Use this form when requesting coverage for all drugs covered under either the pharmacy or medical benefit. Po box 460351 san francisco, ca 94146
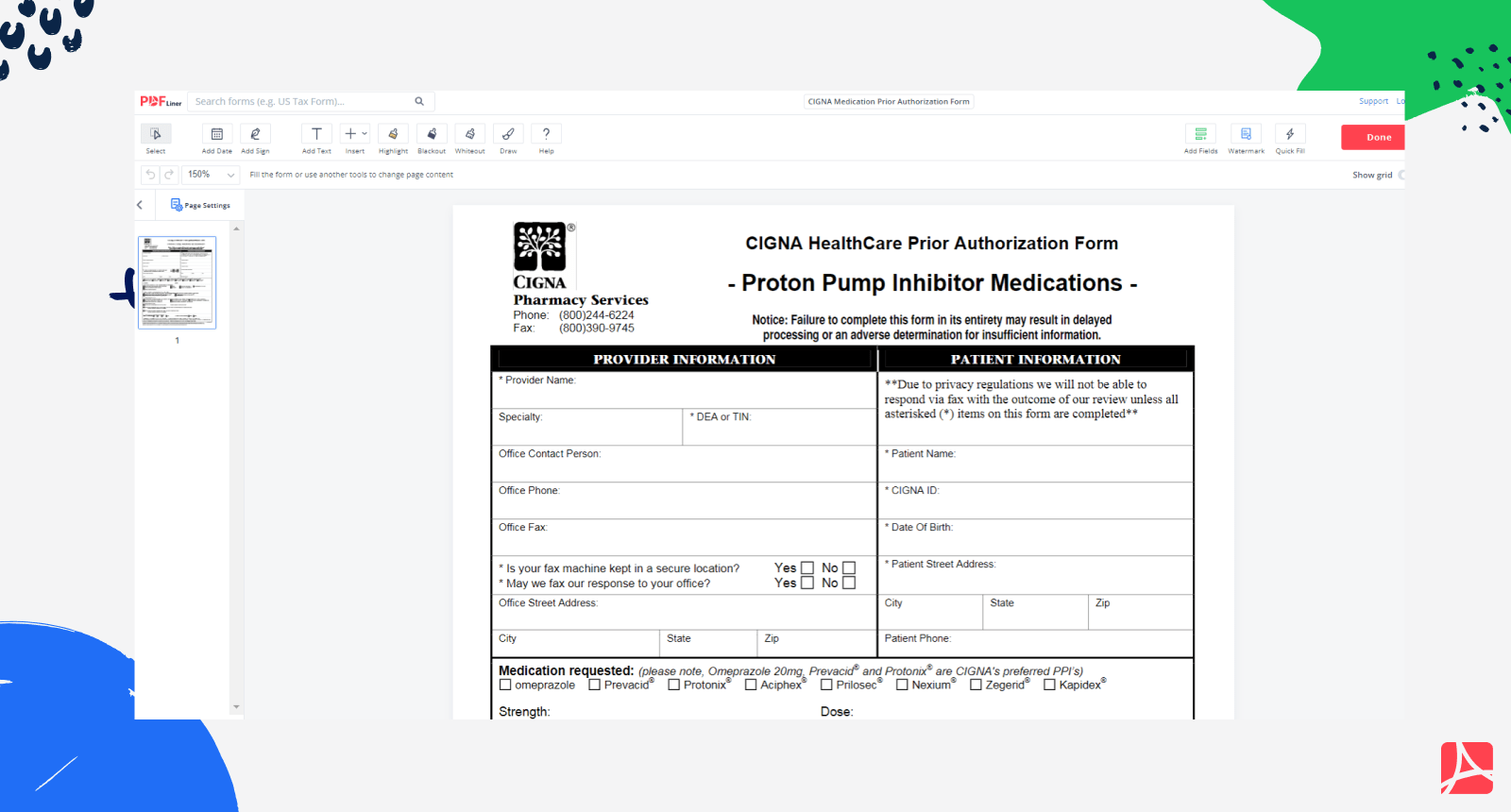
CIGNA Medication Prior Authorization Form PDF blank — PDFliner
If the provider won’t request prior. Use this form when requesting coverage for all drugs covered under either the pharmacy or medical benefit. Po box 460351 san francisco, ca 94146 Your provider can request prior authorization from our health services department by fax, mail, or email. Please complete the form in its.

Alameda alliance authorization form Fill out & sign online DocHub
If the provider won’t request prior. Po box 460351 san francisco, ca 94146 Please complete the form in its. Use this form when requesting coverage for all drugs covered under either the pharmacy or medical benefit. To contact pha or avante behavioral health, please call:

Health Alliance Plan Prior Auth Form
Please complete the form in its. To contact pha or avante behavioral health, please call: Use this form when requesting coverage for all drugs covered under either the pharmacy or medical benefit. Your provider can request prior authorization from our health services department by fax, mail, or email. If the provider won’t request prior.
Fillable Online Pacific Health Alliance Prior Authorization Form Fax
Po box 460351 san francisco, ca 94146 Find forms and resources to better work with us as you care for your patients. If the provider won’t request prior. Please complete the form in its. Your provider can request prior authorization from our health services department by fax, mail, or email.
To Contact Pha Or Avante Behavioral Health, Please Call:
Po box 460351 san francisco, ca 94146 Use this form when requesting coverage for all drugs covered under either the pharmacy or medical benefit. Please complete the form in its. Your provider can request prior authorization from our health services department by fax, mail, or email.
If The Provider Won’t Request Prior.
Find forms and resources to better work with us as you care for your patients.