Refuse Medical Treatment Form
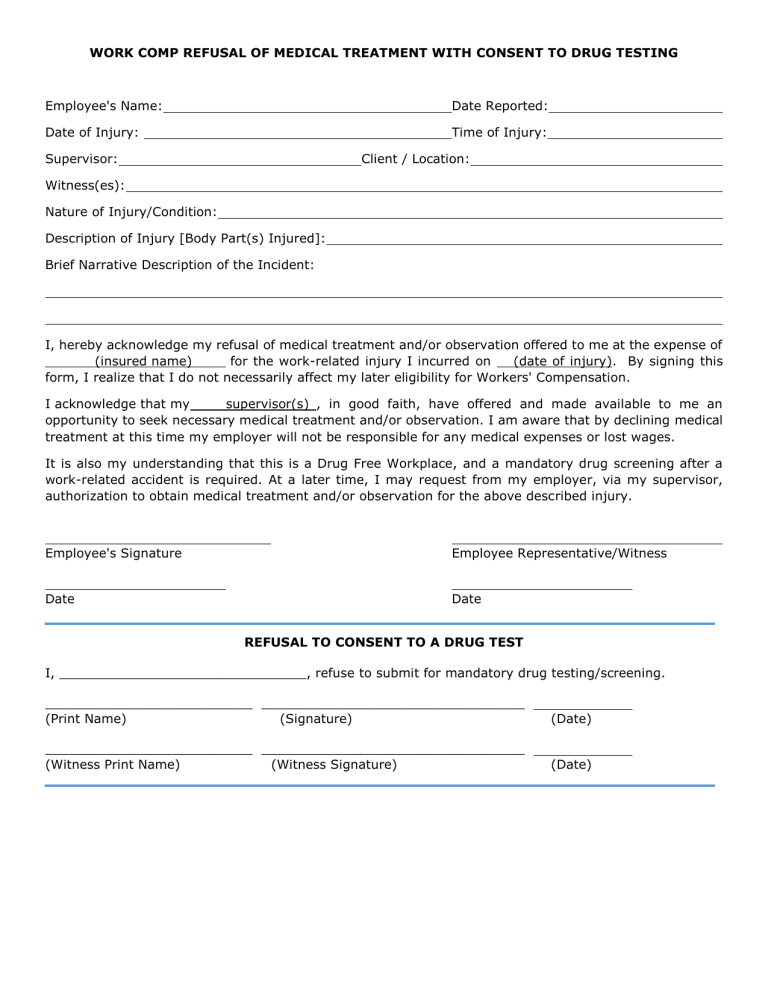
Refuse Medical Treatment Form - My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. Use this form if an employee has a minor injury and they do not feel that they need medical treatment. Medical treatment has been offered to me;. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. If the employee’s injury is obvious, get medical. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.:
Medical treatment has been offered to me;. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. Use this form if an employee has a minor injury and they do not feel that they need medical treatment. If the employee’s injury is obvious, get medical. My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________.
Medical treatment has been offered to me;. My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. Use this form if an employee has a minor injury and they do not feel that they need medical treatment. I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. If the employee’s injury is obvious, get medical.
Fillable Refusal Of Treatment Form printable pdf download
Medical treatment has been offered to me;. My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. If the employee’s injury is obvious, get medical. I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. I, _____, refuse to consent.
Against medical advice form Fill out & sign online DocHub
I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. If the employee’s injury is obvious, get medical. I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the.

Do I have the right to refuse medical treatment? YouTube
By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. Medical treatment has been offered to me;. If the employee’s injury is obvious, get medical. My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described.

Is it a sin to refuse medical treatment?
Medical treatment has been offered to me;. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. Use this form if an employee has.

Refusal of Dental Treatment Form PDF airSlate SignNow
I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. Use this form if an employee has a minor injury and they do not feel that they need medical treatment. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: My.
Medical Treatment Refusal Form Template Amulette
I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: Use this form if an employee has a minor injury and they do not feel that they need medical treatment. I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. By.

Medical Treatment Refusal Form Template amulette
My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. If the employee’s injury is obvious, get medical. Medical treatment has been offered to me;. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: Use this form if an employee has a.
Refusal of Medical Treatment or Observation
Use this form if an employee has a minor injury and they do not feel that they need medical treatment. Medical treatment has been offered to me;. If the employee’s injury is obvious, get medical. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even.

Refusal of Treatment Certificate Competent Person
I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: Use this form if an employee has a minor injury and they do not feel that they need medical treatment. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my.
FREE 43+ Printable Medical Forms in PDF
I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: Medical treatment has been offered to me;. My signature below confirms that i am not experiencing any signs or symptoms resulting.
My Signature Below Confirms That I Am Not Experiencing Any Signs Or Symptoms Resulting From The Incident/Accident Described Above.
I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: If the employee’s injury is obvious, get medical. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. Medical treatment has been offered to me;.
Use This Form If An Employee Has A Minor Injury And They Do Not Feel That They Need Medical Treatment.
I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________.