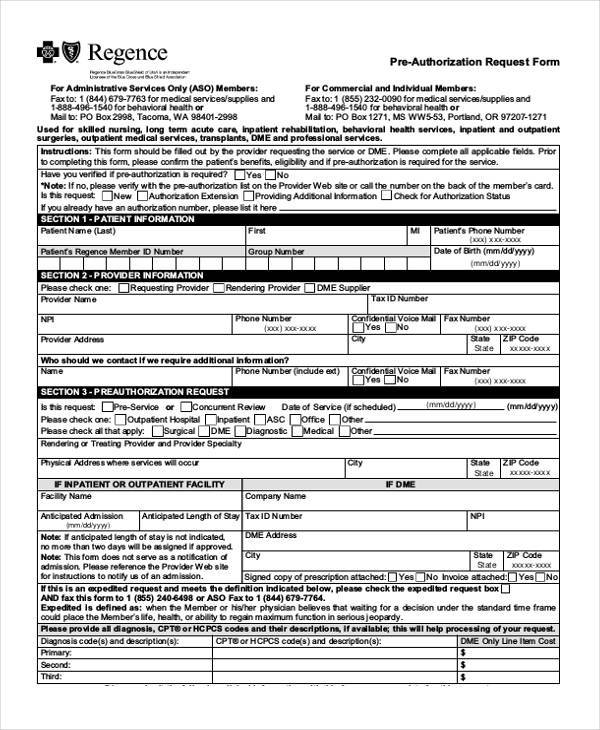
Regence Prior Authorization Form
Regence Prior Authorization Form - Download and print helpful material for. • please note that the below cpt codes are the regence approved cpt codes for aba services. Prior to completing this form, please confirm the patient’s benefits, eligibility. You will need to provide patient, medication, and. Use electronic tools, view lists of. Find out how to get prior authorization for some medications that are not covered by your health plan. Download and fill out this form to request prior authorization for a medication covered by regence. Download the form for your drug and follow. This form should be completed and filled out by the requesting provider. • authorizations are for 6 months (26 weeks).
Download and print helpful material for. Download the form for your drug and follow. • please note that the below cpt codes are the regence approved cpt codes for aba services. • authorizations are for 6 months (26 weeks). Use electronic tools, view lists of. Prior to completing this form, please confirm the patient’s benefits, eligibility. Download and fill out this form to request prior authorization for a medication covered by regence. You will need to provide patient, medication, and. Find out how to get prior authorization for some medications that are not covered by your health plan. This form should be completed and filled out by the requesting provider.
Use electronic tools, view lists of. Find out how to get prior authorization for some medications that are not covered by your health plan. Download and fill out this form to request prior authorization for a medication covered by regence. This form should be completed and filled out by the requesting provider. Download and print helpful material for. You will need to provide patient, medication, and. Prior to completing this form, please confirm the patient’s benefits, eligibility. • please note that the below cpt codes are the regence approved cpt codes for aba services. • authorizations are for 6 months (26 weeks). Download the form for your drug and follow.

Regence Blue Cross Authorization Request ≡ Fill Out Printable PDF Forms
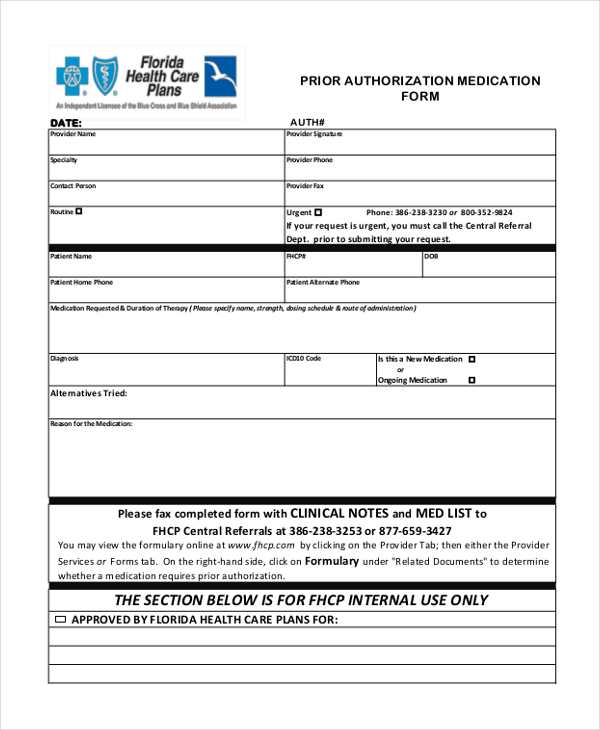
Download the form for your drug and follow. Prior to completing this form, please confirm the patient’s benefits, eligibility. • authorizations are for 6 months (26 weeks). This form should be completed and filled out by the requesting provider. Download and fill out this form to request prior authorization for a medication covered by regence.
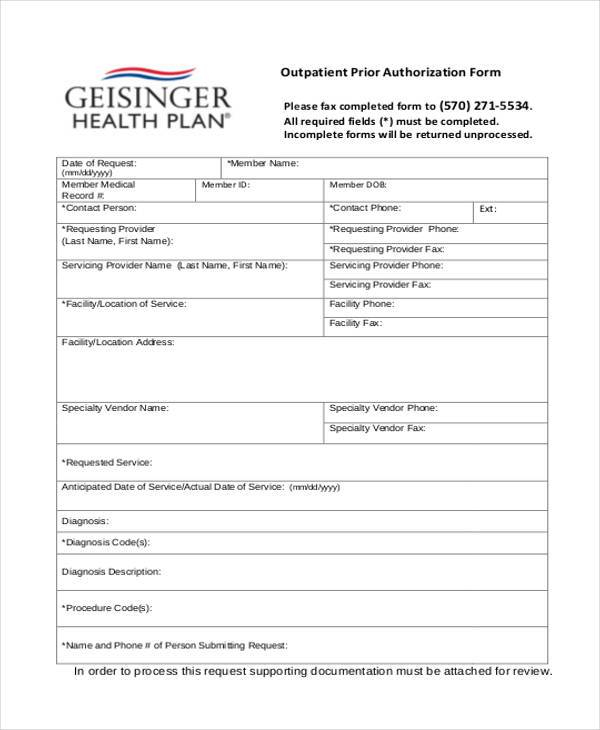
Completing The GHP Prior Authorization Request Form Geisinger
You will need to provide patient, medication, and. Find out how to get prior authorization for some medications that are not covered by your health plan. • please note that the below cpt codes are the regence approved cpt codes for aba services. This form should be completed and filled out by the requesting provider. Download and print helpful material.
Sample Forms For Authorized Drivers / Work authorization sample form
You will need to provide patient, medication, and. Download and print helpful material for. Download the form for your drug and follow. Prior to completing this form, please confirm the patient’s benefits, eligibility. Use electronic tools, view lists of.
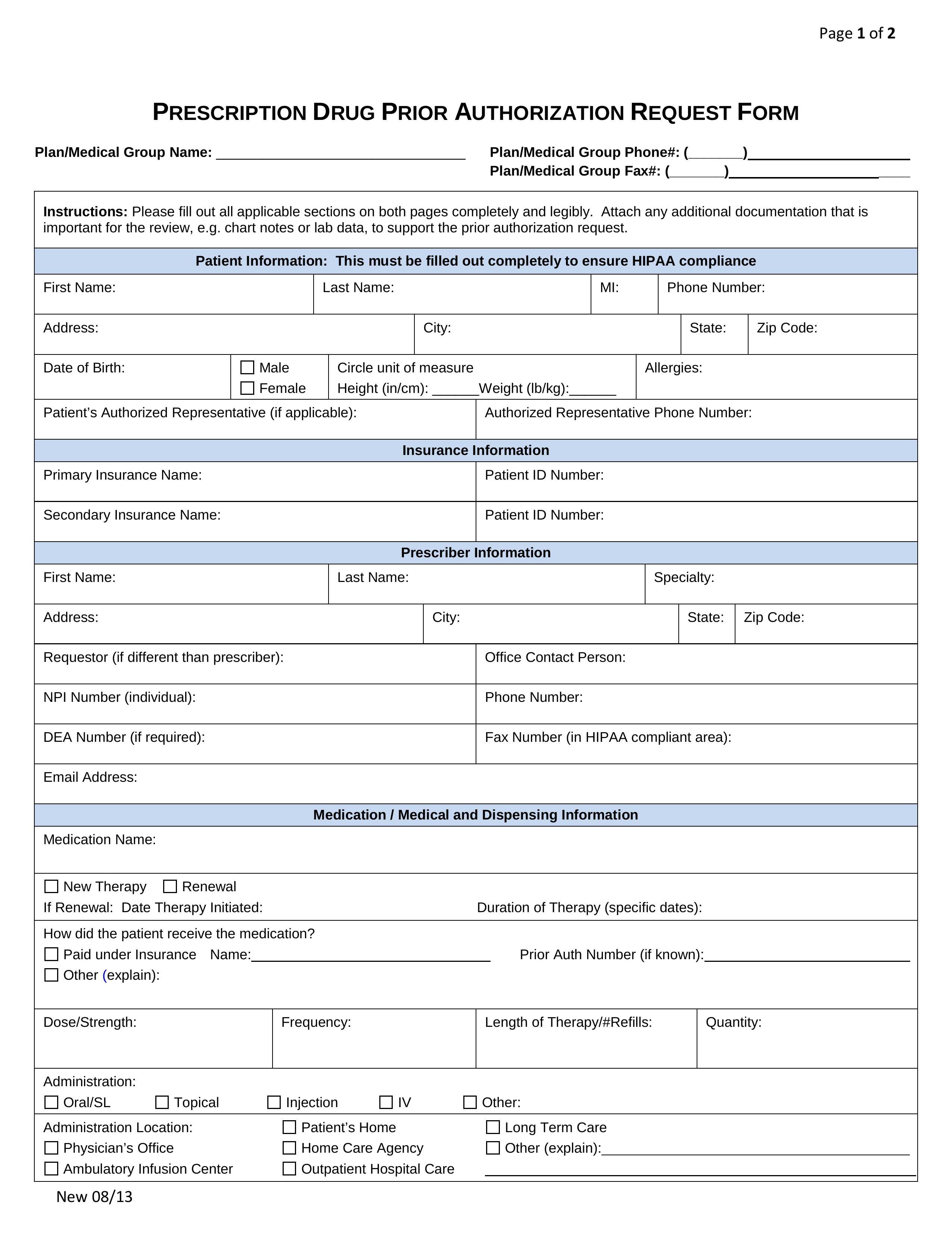
Free Prior (Rx) Authorization Forms PDF eForms
Prior to completing this form, please confirm the patient’s benefits, eligibility. Use electronic tools, view lists of. You will need to provide patient, medication, and. Find out how to get prior authorization for some medications that are not covered by your health plan. This form should be completed and filled out by the requesting provider.
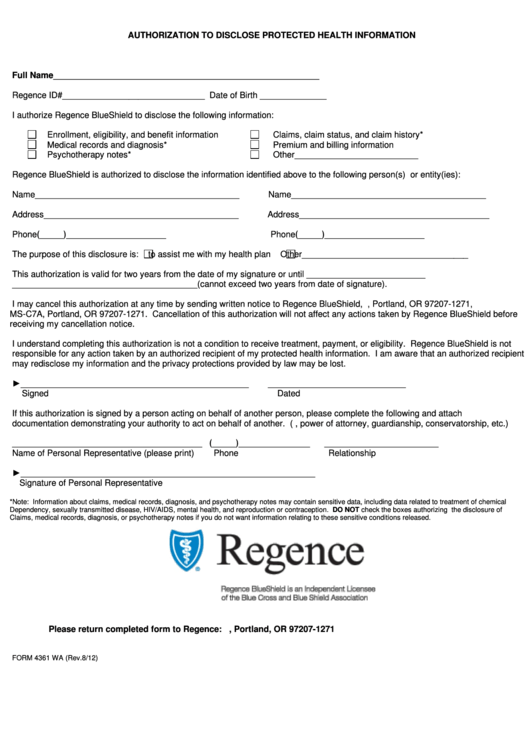
Form 4361 Wa Regence Authorization To Disclose Protected Health
Download and fill out this form to request prior authorization for a medication covered by regence. Download the form for your drug and follow. Prior to completing this form, please confirm the patient’s benefits, eligibility. • authorizations are for 6 months (26 weeks). Use electronic tools, view lists of.
Regence Prior Authorization List 2024 Eddy Nerita
Download and fill out this form to request prior authorization for a medication covered by regence. Use electronic tools, view lists of. Prior to completing this form, please confirm the patient’s benefits, eligibility. This form should be completed and filled out by the requesting provider. • authorizations are for 6 months (26 weeks).
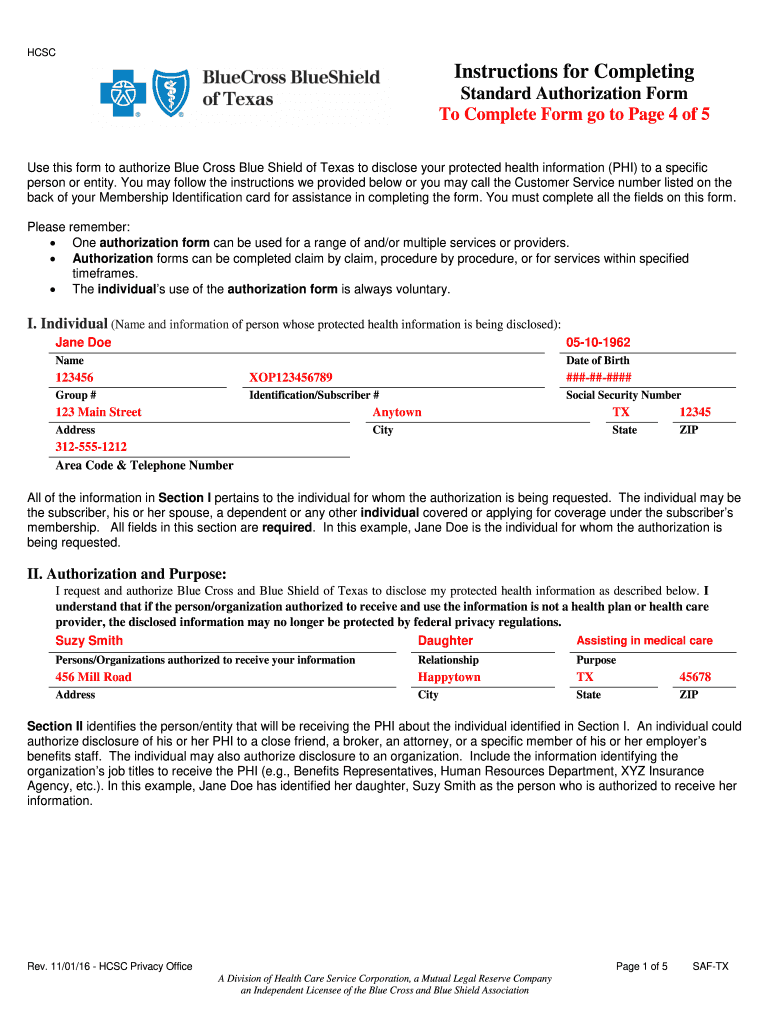
Standard authorization form bcbs Fill out & sign online DocHub
You will need to provide patient, medication, and. Use electronic tools, view lists of. Download and fill out this form to request prior authorization for a medication covered by regence. Prior to completing this form, please confirm the patient’s benefits, eligibility. Download and print helpful material for.
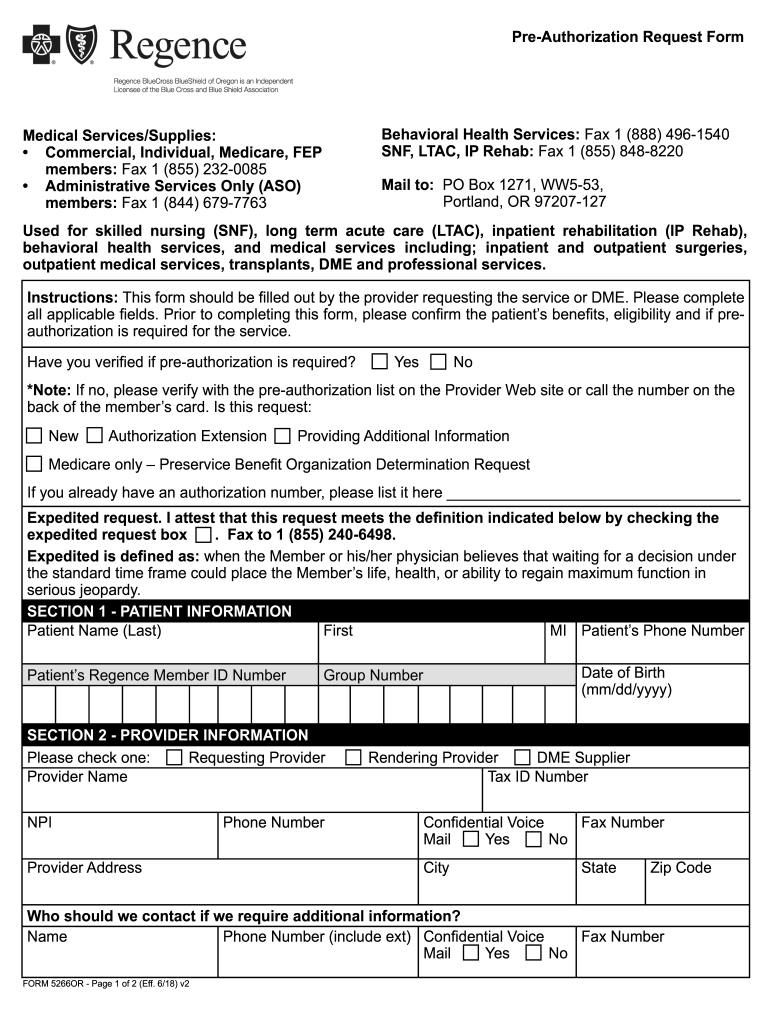
Regence Prior Authorization PDF 20182024 Form Fill Out and Sign
Prior to completing this form, please confirm the patient’s benefits, eligibility. • authorizations are for 6 months (26 weeks). This form should be completed and filled out by the requesting provider. Use electronic tools, view lists of. Download the form for your drug and follow.

2012 Form Regence PD019Fill Online, Printable, Fillable, Blank pdfFiller
Use electronic tools, view lists of. This form should be completed and filled out by the requesting provider. • authorizations are for 6 months (26 weeks). Prior to completing this form, please confirm the patient’s benefits, eligibility. You will need to provide patient, medication, and.

Healthfirst Leaf Plans Prior Authorization Forms
• authorizations are for 6 months (26 weeks). Download and fill out this form to request prior authorization for a medication covered by regence. You will need to provide patient, medication, and. Download and print helpful material for. Prior to completing this form, please confirm the patient’s benefits, eligibility.
Download The Form For Your Drug And Follow.
Find out how to get prior authorization for some medications that are not covered by your health plan. This form should be completed and filled out by the requesting provider. Download and print helpful material for. Download and fill out this form to request prior authorization for a medication covered by regence.
• Please Note That The Below Cpt Codes Are The Regence Approved Cpt Codes For Aba Services.
You will need to provide patient, medication, and. Prior to completing this form, please confirm the patient’s benefits, eligibility. Use electronic tools, view lists of. • authorizations are for 6 months (26 weeks).