Signature On File Form
Signature On File Form - I hereby authorize jefferson university physicians to disclose to my insurance company(s) copies of my medical records(s) to obtain payment for. I also understand that i am. If a patient is eligible for coverage under two or more dental care programs, the primary insurance is. Signature on file form • i understand that my insurance is an agreement between my insurance company and me. Woodlands healing research center integrative family medicine 5724 clymer rd. Patient/guardian signature _____ date ___/___/_____ ~authorization to release medical information~ i authorize any holder. This form captures the signature and. Authorize a copy of this “signature on file” form to be used in place of the original and that this copy may be used on all my insurance submissions.
Signature on file form • i understand that my insurance is an agreement between my insurance company and me. Woodlands healing research center integrative family medicine 5724 clymer rd. Authorize a copy of this “signature on file” form to be used in place of the original and that this copy may be used on all my insurance submissions. Patient/guardian signature _____ date ___/___/_____ ~authorization to release medical information~ i authorize any holder. If a patient is eligible for coverage under two or more dental care programs, the primary insurance is. I hereby authorize jefferson university physicians to disclose to my insurance company(s) copies of my medical records(s) to obtain payment for. I also understand that i am. This form captures the signature and.
Signature on file form • i understand that my insurance is an agreement between my insurance company and me. Authorize a copy of this “signature on file” form to be used in place of the original and that this copy may be used on all my insurance submissions. This form captures the signature and. Woodlands healing research center integrative family medicine 5724 clymer rd. I also understand that i am. If a patient is eligible for coverage under two or more dental care programs, the primary insurance is. I hereby authorize jefferson university physicians to disclose to my insurance company(s) copies of my medical records(s) to obtain payment for. Patient/guardian signature _____ date ___/___/_____ ~authorization to release medical information~ i authorize any holder.
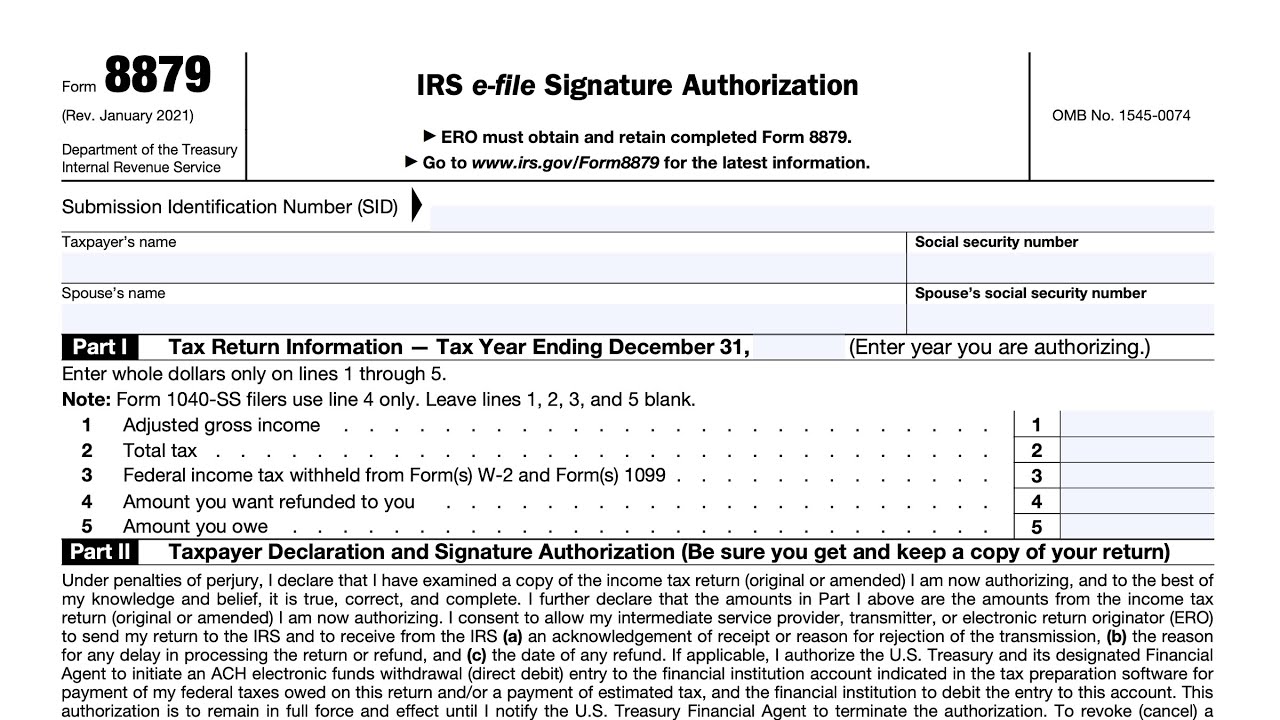
Downloadable Form 8879 IRS EFile Signature Authorization, 42 OFF
Woodlands healing research center integrative family medicine 5724 clymer rd. Authorize a copy of this “signature on file” form to be used in place of the original and that this copy may be used on all my insurance submissions. Patient/guardian signature _____ date ___/___/_____ ~authorization to release medical information~ i authorize any holder. I also understand that i am. Signature.

Signature on File
If a patient is eligible for coverage under two or more dental care programs, the primary insurance is. Patient/guardian signature _____ date ___/___/_____ ~authorization to release medical information~ i authorize any holder. Authorize a copy of this “signature on file” form to be used in place of the original and that this copy may be used on all my insurance.
Signature files
This form captures the signature and. Woodlands healing research center integrative family medicine 5724 clymer rd. I also understand that i am. I hereby authorize jefferson university physicians to disclose to my insurance company(s) copies of my medical records(s) to obtain payment for. If a patient is eligible for coverage under two or more dental care programs, the primary insurance.

Signature Form Fill and Sign Printable Template Online US Legal Forms
I hereby authorize jefferson university physicians to disclose to my insurance company(s) copies of my medical records(s) to obtain payment for. I also understand that i am. Patient/guardian signature _____ date ___/___/_____ ~authorization to release medical information~ i authorize any holder. Woodlands healing research center integrative family medicine 5724 clymer rd. If a patient is eligible for coverage under two.
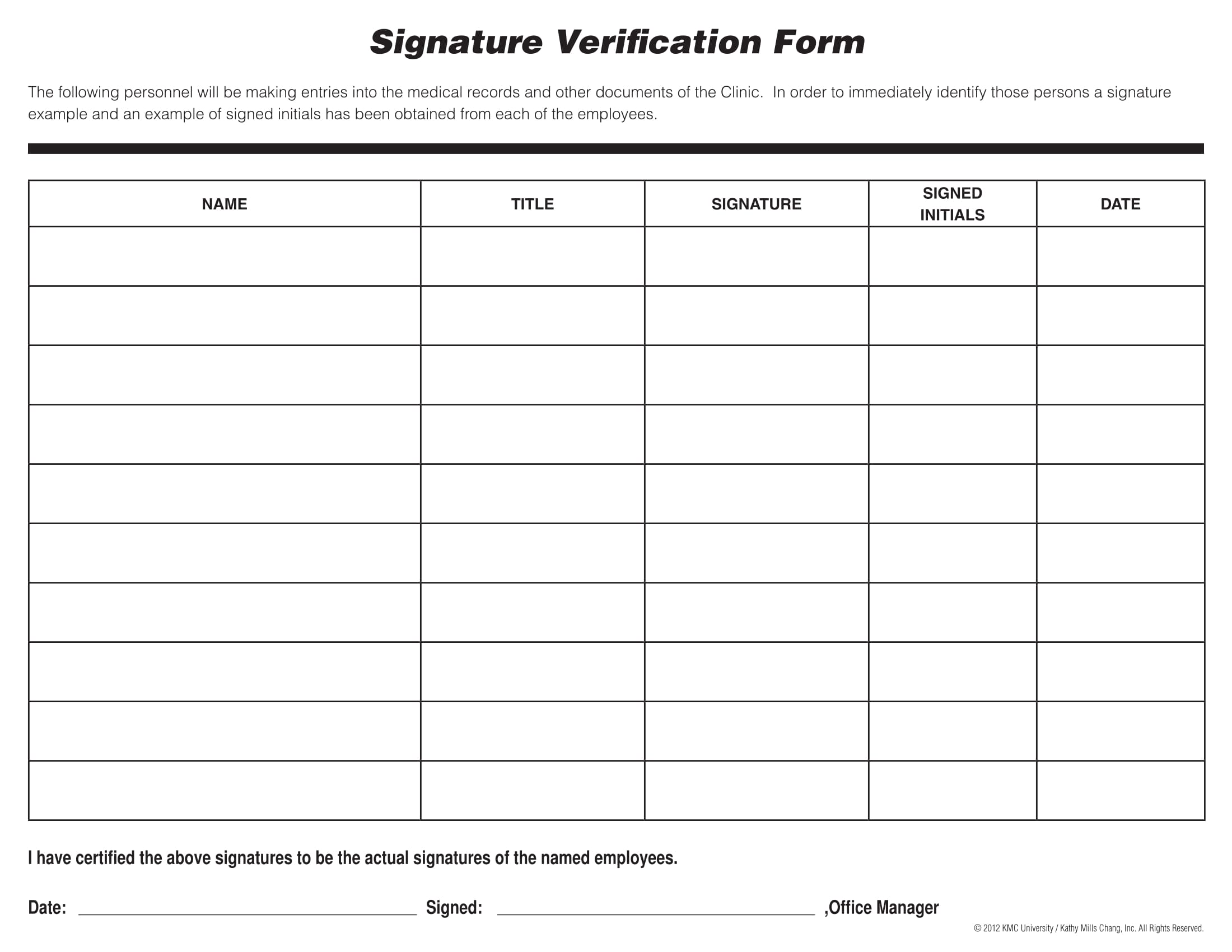
Free 13+ Signature Verification Form Samples, PDF, MS Word, Google Docs,
I also understand that i am. Woodlands healing research center integrative family medicine 5724 clymer rd. Patient/guardian signature _____ date ___/___/_____ ~authorization to release medical information~ i authorize any holder. This form captures the signature and. Authorize a copy of this “signature on file” form to be used in place of the original and that this copy may be used.
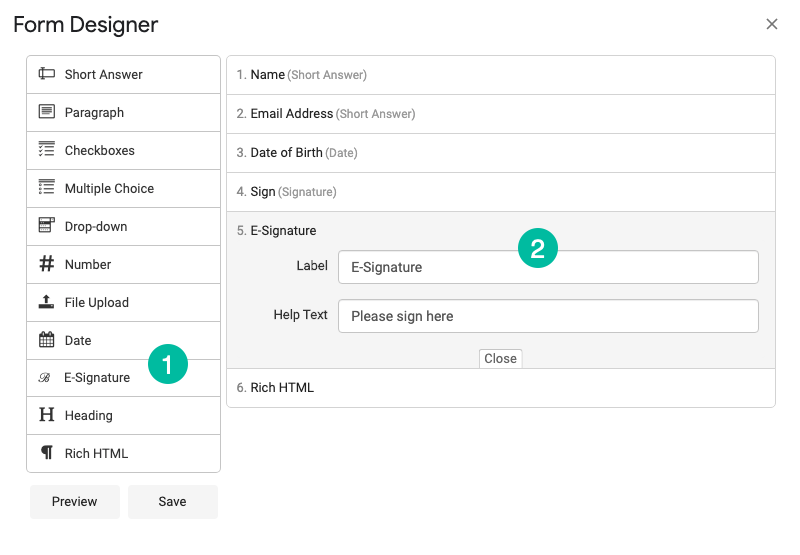
How to Create an Online Form with Electronic Signature Digital
Woodlands healing research center integrative family medicine 5724 clymer rd. This form captures the signature and. Authorize a copy of this “signature on file” form to be used in place of the original and that this copy may be used on all my insurance submissions. Patient/guardian signature _____ date ___/___/_____ ~authorization to release medical information~ i authorize any holder. Signature.
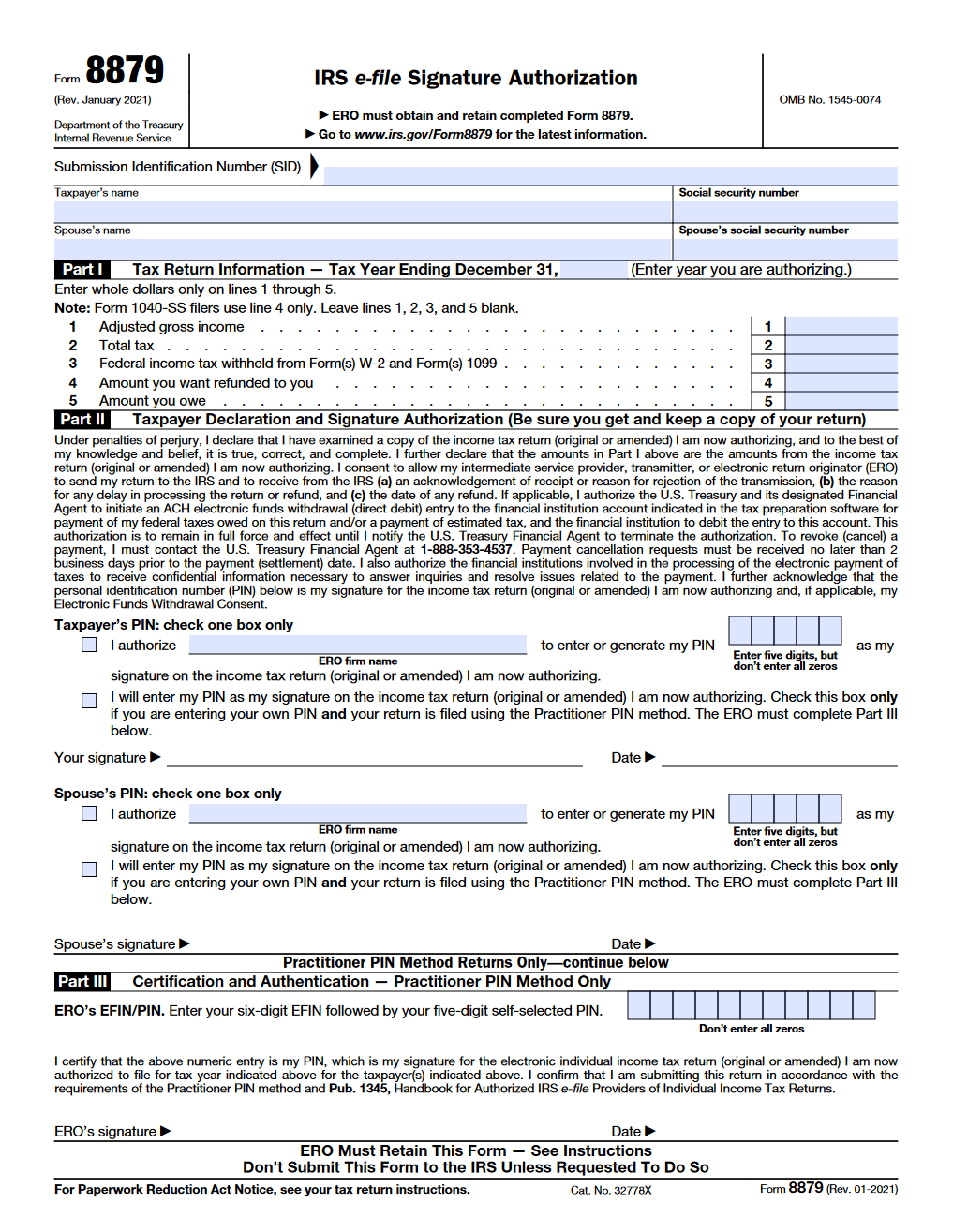
IRS Form 8879. IRS efile Signature Authorization Forms Docs 2023
Woodlands healing research center integrative family medicine 5724 clymer rd. If a patient is eligible for coverage under two or more dental care programs, the primary insurance is. Signature on file form • i understand that my insurance is an agreement between my insurance company and me. Authorize a copy of this “signature on file” form to be used in.

Signature File Office and School Supplies YAHYERA.AE
This form captures the signature and. Authorize a copy of this “signature on file” form to be used in place of the original and that this copy may be used on all my insurance submissions. Patient/guardian signature _____ date ___/___/_____ ~authorization to release medical information~ i authorize any holder. If a patient is eligible for coverage under two or more.

Create pdf form with electronic signature ressfield
Woodlands healing research center integrative family medicine 5724 clymer rd. I also understand that i am. This form captures the signature and. Authorize a copy of this “signature on file” form to be used in place of the original and that this copy may be used on all my insurance submissions. Patient/guardian signature _____ date ___/___/_____ ~authorization to release medical.
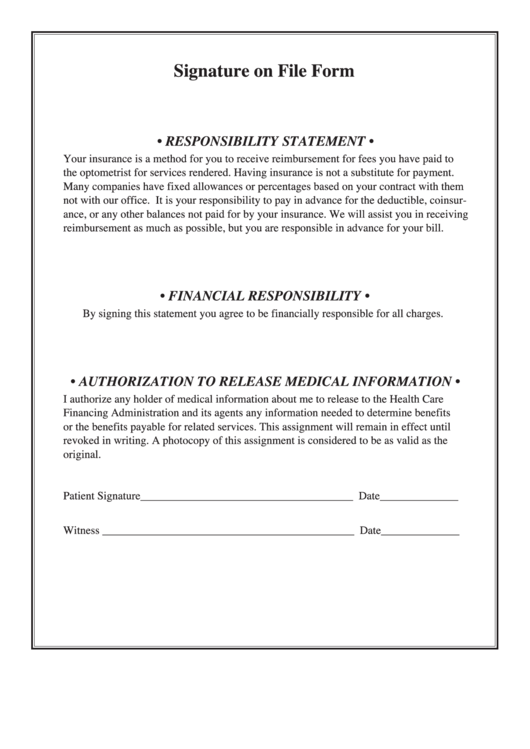
Signature On File Form & Authorization To Release Medical Information
I also understand that i am. If a patient is eligible for coverage under two or more dental care programs, the primary insurance is. Authorize a copy of this “signature on file” form to be used in place of the original and that this copy may be used on all my insurance submissions. Patient/guardian signature _____ date ___/___/_____ ~authorization to.
I Also Understand That I Am.
This form captures the signature and. Signature on file form • i understand that my insurance is an agreement between my insurance company and me. Authorize a copy of this “signature on file” form to be used in place of the original and that this copy may be used on all my insurance submissions. Woodlands healing research center integrative family medicine 5724 clymer rd.
I Hereby Authorize Jefferson University Physicians To Disclose To My Insurance Company(S) Copies Of My Medical Records(S) To Obtain Payment For.
Patient/guardian signature _____ date ___/___/_____ ~authorization to release medical information~ i authorize any holder. If a patient is eligible for coverage under two or more dental care programs, the primary insurance is.